Explore how culture, PCR, CRP, procalcitonin and newer host-response tests help distinguish bacterial from viral infections, while supporting safer antibiotic use and antimicrobial stewardship.
Bacterial and viral infections can produce remarkably similar symptoms. Fever, cough, fatigue, headache, raised inflammatory markers and general malaise may occur in both. A patient who appears to have a straightforward viral respiratory illness may have a bacterial infection, while another patient with a high temperature and raised C-reactive protein may not require antibiotics.
This uncertainty creates an important clinical question:
Is the infection bacterial, viral, mixed, or caused by something else entirely?
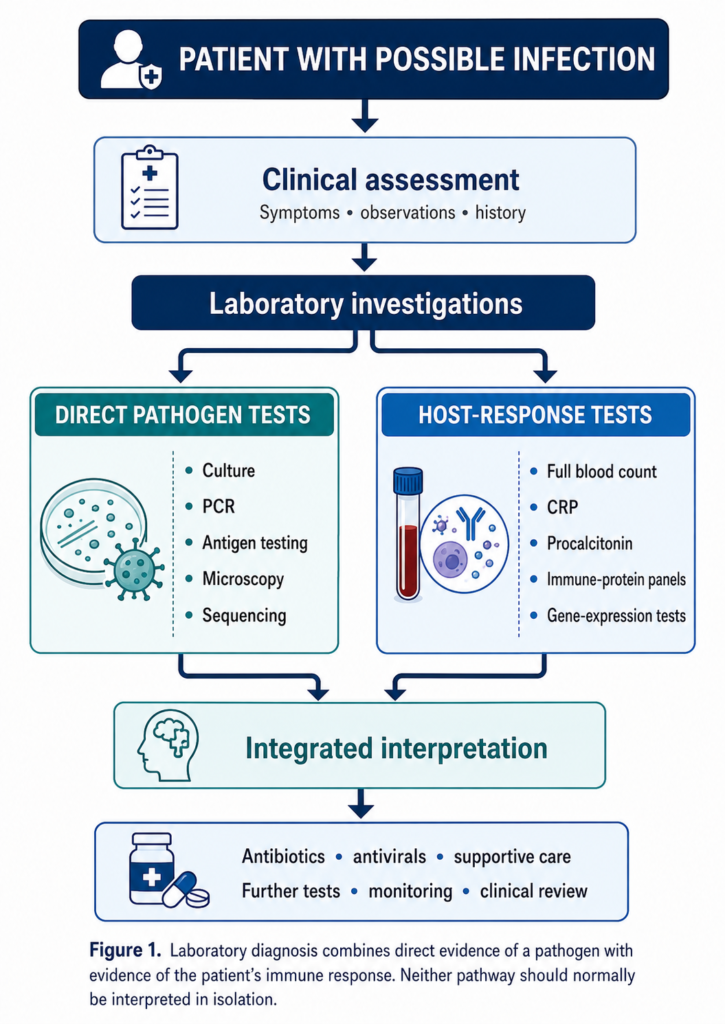
Laboratory testing helps clinicians answer this question by looking for the pathogen itself and by measuring how the patient’s immune system is responding. However, no single laboratory result can provide a perfect answer in every patient.
Modern diagnostic practice therefore combines clinical assessment, direct pathogen detection, inflammatory biomarkers, host-response testing and professional judgement.
This article explains how these tests work, their strengths and limitations, and how they support antimicrobial stewardship.
Educational notice: This article is intended for biomedical science education and public awareness. Laboratory results must be interpreted by appropriately qualified healthcare professionals within the individual clinical context.
Why is it difficult to distinguish bacterial from viral infection?
Bacteria and viruses are biologically different.
Bacteria are living, single-celled microorganisms that can reproduce independently under suitable conditions. Viruses are smaller infectious agents containing genetic material enclosed within a protein coat. They must enter host cells and use cellular machinery to reproduce.
Despite these differences, the human immune system may produce similar early responses to both types of infection. These can include:
- fever;
- increased heart rate;
- cough or breathlessness;
- headache;
- muscle pain;
- fatigue;
- raised white blood cell count;
- increased C-reactive protein;
- general inflammation.
The same symptoms can also occur in non-infectious conditions, including autoimmune disease, malignancy, trauma, pulmonary embolism and inflammatory disorders.
Furthermore, patients can have bacterial and viral infections simultaneously. For example, a viral respiratory infection may damage the respiratory epithelium and increase susceptibility to secondary bacterial pneumonia.
The question is therefore not always a simple choice between bacterial and viral infection.
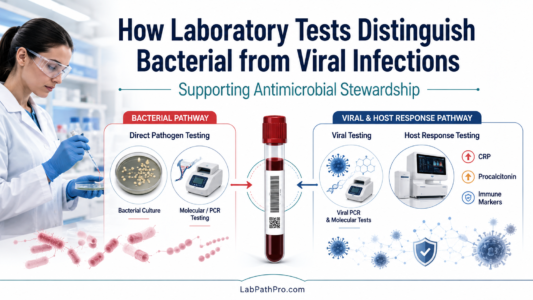
Two main laboratory approaches
Laboratory investigations can be divided broadly into two approaches.
- Pathogen-directed testing
These methods search directly for the microorganism or its components.
Examples include:
- bacterial culture;
- microscopy;
- antigen detection;
- polymerase chain reaction;
- multiplex molecular panels;
- microbial sequencing.
- Host-response testing
These methods examine the patient’s biological response to infection.
Examples include:
- white blood cell count;
- neutrophil and lymphocyte measurements;
- C-reactive protein;
- procalcitonin;
- cytokine and immune-protein signatures;
- host gene-expression tests.
The two approaches provide different information and are usually complementary.
Direct pathogen detection
Bacterial culture
Culture remains a fundamental part of microbiology. A sample is inoculated onto suitable culture media and incubated under controlled conditions. Any organisms that grow can then be identified.
Common samples include:
- blood;
- urine;
- cerebrospinal fluid;
- sputum;
- wound swabs;
- faeces;
- tissue;
- respiratory samples.
Culture has a major advantage: it detects viable organisms and may allow antimicrobial susceptibility testing.
This can help determine which antibiotics are likely to be effective and identify resistance mechanisms.
However, culture also has limitations.
Results may take several hours or days, depending on the organism. Previous antibiotic treatment can reduce organism recovery. Some bacteria are difficult to culture, require specialised conditions or may be present in very small numbers.
The presence of bacteria does not always prove that they are causing disease. Some samples may contain normal flora, colonising organisms or environmental contaminants.
For example, bacteria grown from a poorly collected sputum sample may reflect organisms from the mouth rather than a lower respiratory tract infection.
Blood cultures
Blood cultures are particularly important in suspected bloodstream infection and sepsis.
Blood is collected into aerobic and anaerobic bottles and incubated within an automated monitoring system. Microbial growth produces measurable changes that trigger an alert.
Positive bottles undergo further testing, including:
- Gram staining;
- subculture;
- organism identification;
- antimicrobial susceptibility testing;
- molecular resistance testing where appropriate.
Blood culture results can directly influence patient treatment. However, sensitivity may be affected by:
- inadequate blood volume;
- collection after antibiotics have started;
- intermittent bacteraemia;
- slow-growing or fastidious organisms;
- contamination during collection.
For Biomedical Scientists, correct specimen collection, transport, loading, incubation, identification and result escalation are essential components of the diagnostic pathway.
Polymerase chain reaction
Polymerase chain reaction, usually abbreviated to PCR, detects selected microbial DNA or RNA.
For RNA viruses, such as influenza viruses or SARS-CoV-2, the RNA is first converted into complementary DNA before amplification.
PCR can detect pathogens much faster than traditional culture and may remain positive when only a small amount of microbial genetic material is present.
Multiplex PCR panels can test for several organisms in a single sample. Respiratory panels may include combinations of:
- influenza A and B;
- respiratory syncytial virus;
- SARS-CoV-2;
- adenovirus;
- rhinovirus or enterovirus;
- parainfluenza viruses;
- selected bacterial respiratory pathogens.
However, a positive molecular result must be interpreted carefully.
PCR detects genetic material. It may not confirm that the organism is viable or actively causing the patient’s symptoms. Genetic material can sometimes remain detectable after an infection has resolved.
Detection of a virus also does not automatically exclude bacterial co-infection.
Many molecular panels provide limited information about antimicrobial susceptibility. Culture may still be required for full identification, resistance testing and public health surveillance.
Antigen tests
Antigen tests detect specific microbial proteins. They are often faster and technically simpler than molecular testing. Examples include tests for influenza, SARS-CoV-2, group A streptococcus and certain gastrointestinal pathogens.
The main limitation is that some antigen tests are less sensitive than laboratory-based molecular methods. A negative result may therefore require confirmation when clinical suspicion remains high.
Host-response biomarkers
Direct testing asks:
Can we find the organism?
Host-response testing asks:
How is the patient’s immune system reacting?
Host-response markers can be useful when the causative organism has not been identified, the sample is difficult to obtain or the clinical presentation remains uncertain.
However, these markers are rarely specific enough to identify an exact pathogen.
Full blood count and white cell differential
A full blood count provides information about the number and distribution of circulating blood cells.
Neutrophils
Neutrophilia is commonly associated with bacterial infection. Neutrophils are rapidly recruited to areas of tissue damage and bacterial invasion, where they engulf microorganisms and release antimicrobial substances.
However, neutrophilia can also occur because of:
- inflammation;
- physical stress;
- corticosteroid treatment;
- tissue injury;
- smoking;
- malignancy;
- pregnancy.
A normal neutrophil count does not exclude serious bacterial infection.
Lymphocytes
Some viral infections are associated with lymphocytosis or characteristic reactive lymphocytes.
However, viral infections may also produce lymphopenia, particularly in severe disease. The direction and size of the change depend on the virus, illness stage and patient factors.
The white cell differential is therefore supportive evidence rather than a definitive bacterial-versus-viral test.
C-reactive protein
C-reactive protein, or CRP, is an acute-phase protein produced mainly by the liver in response to inflammatory cytokines.
CRP concentrations can increase substantially during infection and tissue inflammation. It is widely available, relatively inexpensive and frequently used to monitor changes over time.
Higher CRP concentrations may increase suspicion of bacterial infection, but CRP is not specific for bacteria.
CRP may also rise in:
- severe viral infections;
- autoimmune disease;
- inflammatory disorders;
- malignancy;
- surgery;
- trauma;
- tissue necrosis.
The timing of sampling is important. CRP may remain low during the early stage of infection before increasing later.
Serial results can sometimes be more informative than a single measurement because they show whether inflammation is increasing, remaining stable or resolving.
NICE guidance on CRP
For adults with suspected lower respiratory tract infection, the National Institute for Health and Care Excellence advises considering point-of-care CRP testing when the need for antibiotics remains unclear after clinical assessment.
Within that specific pathway:
- a CRP concentration above 100 mg/L supports offering immediate antibiotics;
- a concentration between 20 and 100 mg/L supports considering a back-up antibiotic prescription;
- a concentration below 20 mg/L supports not routinely offering antibiotics.
These thresholds apply to the defined adult lower respiratory tract infection pathway. They should not be applied automatically to every patient, age group, sample type or suspected infection.
Procalcitonin
Procalcitonin is a precursor of the hormone calcitonin. In healthy people, circulating concentrations are usually low. During systemic bacterial infection, procalcitonin production can increase in several tissues in response to inflammatory signals and bacterial products.
Many viral immune responses involve interferon signalling, which may suppress procalcitonin production. This is one reason why procalcitonin can provide additional information when bacterial infection is suspected.
Potential uses include:
- assessment of suspected bacterial respiratory infection;
- support for antimicrobial stewardship;
- monitoring the response to treatment;
- assisting decisions about stopping antibiotics in selected patients.
However, procalcitonin is not a perfect bacterial marker.
It may remain low in:
- early infection;
- localised bacterial infection;
- certain atypical infections;
- some immunocompromised patients.
It may rise in the absence of bacterial infection because of:
- major surgery;
- severe trauma;
- burns;
- cardiogenic shock;
- prolonged circulatory failure;
- some malignancies;
- impaired renal function.
Evidence from randomised trials indicates that procalcitonin-guided pathways can reduce antibiotic exposure in selected patients with acute respiratory infections. Nevertheless, success depends on the clinical setting, the algorithm used and whether healthcare professionals follow the agreed pathway.
Procalcitonin should therefore support clinical decision-making rather than replace it.
Modern multi-protein host-response testing
Single biomarkers such as CRP and procalcitonin provide useful but incomplete information.
Newer tests combine several immune-response proteins and use an algorithm to interpret the overall pattern.
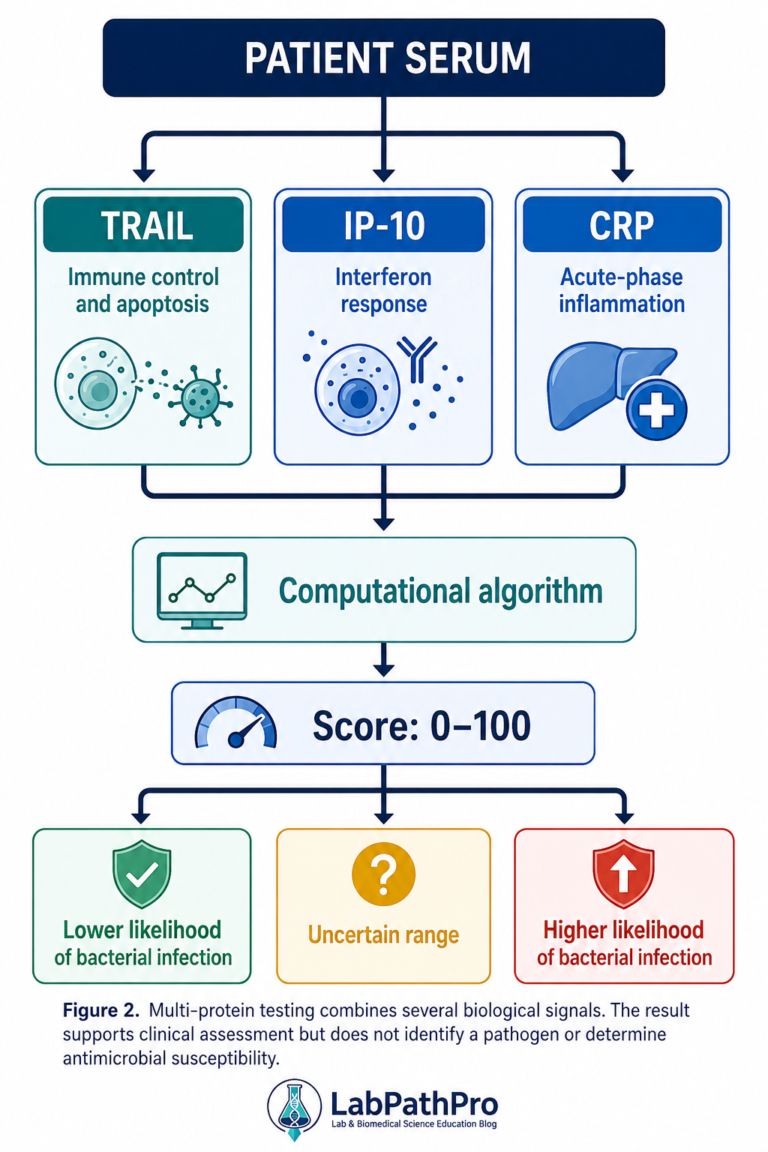
TRAIL, IP-10 and CRP
One modern host-response approach measures:
TRAIL
Tumour necrosis factor-related apoptosis-inducing ligand, known as TRAIL, is involved in immune regulation and programmed cell death. Its pattern may differ between bacterial and viral immune responses.
IP-10
Interferon-gamma-induced protein 10, also called CXCL10, is a signalling protein associated with interferon-driven immune activity. It may become particularly relevant during viral infection.
CRP
CRP adds information about the strength and pattern of systemic inflammation.
The three proteins provide more information together than any one marker alone.
MeMed BV
MeMed BV is an example of a multi-protein host-response test.
The assay measures TRAIL, IP-10 and CRP in serum. A computational algorithm combines the measurements and produces a numerical score between 0 and 100.
Lower scores are associated with a response more consistent with viral infection. Higher scores indicate an increasing likelihood of bacterial infection. Intermediate categories reflect greater diagnostic uncertainty.
Importantly, this is one combined score. It does not identify the individual bacterium or virus and does not provide antimicrobial susceptibility results.
The United States Food and Drug Administration cleared the test as an aid for use alongside clinical assessment and other laboratory findings in defined adult and paediatric emergency or urgent-care populations with suspected acute infection.
Studies in children and adults have reported encouraging diagnostic performance. However, performance varies according to patient selection, disease prevalence, immune status, illness severity and the reference method used to classify infection.
The assay should not be assumed to work identically in intensive care, immunocompromised patients, prolonged illness or populations outside its validated intended use.
Host gene-expression testing
The next generation of host-response tests measures changes in messenger RNA within the patient’s blood cells.
When the immune system encounters a pathogen, specific genes become more or less active. The resulting gene-expression pattern can provide information about whether the immune response is more consistent with:
- bacterial infection;
- viral infection;
- non-infectious inflammation;
- a higher risk of severe illness.
TriVerity
TriVerity is an example of a rapid host gene-expression test cleared by the United States Food and Drug Administration in 2025.
The system measures the relative expression of 29 informative host-response RNA transcripts, along with housekeeping genes and process controls.
It uses reverse-transcription loop-mediated isothermal amplification and produces three separate scores relating to:
- bacterial infection;
- viral infection;
- likelihood of severe illness.
The severe illness assessment considers the likelihood of needing mechanical ventilation, vasopressor support or renal replacement therapy within seven days in its intended adult emergency-department population.
Results are produced in approximately 30 minutes.
This technology represents an important development because it attempts to distinguish infection type while also assessing illness severity.
However, regulatory clearance in one country does not automatically mean that a test is available, recommended or validated for routine NHS use. Local verification, clinical evaluation, governance, cost-effectiveness assessment and integration into established pathways would still be required.
Comparing the main laboratory approaches
|
Test or method |
What it measures |
Main strength |
Important limitation |
|
Bacterial culture |
Growth of viable organisms |
Identification and susceptibility testing |
May take days and can be affected by antibiotics |
|
PCR |
Microbial DNA or RNA |
Rapid and sensitive pathogen detection |
May detect colonisation or residual genetic material |
|
Antigen testing |
Microbial proteins |
Rapid and accessible |
Sensitivity may be lower than molecular testing |
|
Full blood count |
Blood cell numbers and distribution |
Widely available and inexpensive |
Patterns are non-specific |
|
CRP |
Acute-phase inflammatory response |
Useful for assessing and monitoring inflammation |
Cannot reliably distinguish all bacterial and viral infections |
|
Procalcitonin |
Host response associated with systemic bacterial infection |
Can support stewardship pathways |
Affected by timing, severity and non-infectious conditions |
|
TRAIL/IP-10/CRP panel |
Combined host protein response |
Integrates several immune pathways |
Does not identify the organism or resistance |
|
Host gene-expression test |
Immune-cell RNA expression |
Can provide diagnostic and prognostic scores |
Requires specialised technology and population-specific validation |
Why no single result should be used alone
Every laboratory test has a defined intended use, uncertainty and risk of error.
A positive viral PCR result does not always prove that the virus is responsible for all the patient’s symptoms. A patient may have a secondary bacterial infection.
A raised CRP does not automatically mean that antibiotics are required.
A low procalcitonin does not completely exclude bacterial infection, particularly if the illness is early or localised.
A high host-response score does not identify the responsible organism or indicate which antibiotic should be prescribed.
Clinical decisions should consider:
- symptoms and illness duration;
- examination findings;
- physiological observations;
- patient age;
- comorbidities;
- immune status;
- recent antimicrobial treatment;
- infection site;
- imaging;
- microbiology;
- biomarker trends;
- local prevalence and resistance patterns.
The safest interpretation is based on the complete diagnostic picture.
Pre-analytical and analytical considerations
For trainee Biomedical Scientists, it is important to recognise that test accuracy begins before the sample reaches the analyser.
Patient identification
Incorrect identification can lead to a result being assigned to the wrong patient, creating an immediate risk of inappropriate treatment.
Sample timing
Biomarker concentrations and pathogen loads change during infection. A sample collected very early may produce a different result from one collected later.
Sample type
Serum, plasma, whole blood, respiratory secretions and cerebrospinal fluid are not interchangeable. Each assay must be performed using the validated specimen type.
Transport and storage
Delays, unsuitable temperatures, incorrect containers and poor handling may affect cell stability, RNA integrity, microbial viability or biomarker concentrations.
Contamination
Contaminated cultures can result in unnecessary antibiotic treatment, further testing and prolonged hospital admission.
Quality control
Laboratories must use internal quality-control procedures to monitor analytical performance and participate in appropriate external quality-assessment schemes where available.
Verification and validation
Before implementation, laboratories should confirm that the assay performs acceptably within the local environment.
This may include assessment of:
- precision;
- bias;
- reportable range;
- analytical sensitivity;
- analytical specificity;
- interference;
- sample stability;
- carryover;
- reference or decision limits;
- comparison with an established method;
- performance within the intended clinical population.
Algorithm-based tests require additional governance. Changes to software, interpretation rules or classifier versions may alter results even when the physical analyser remains unchanged.
Antimicrobial stewardship
Antimicrobial stewardship is a coordinated approach to promoting and monitoring the appropriate use of antimicrobial medicines.
The aim is to ensure that patients who need antibiotics receive effective treatment while reducing unnecessary or inappropriate exposure.
Unnecessary antibiotic use can:
- expose patients to adverse effects;
- disrupt the normal microbiome;
- increase the risk of Clostridioides difficile infection;
- encourage antimicrobial resistance;
- make future infections more difficult to treat;
- increase healthcare costs.
According to NICE, antimicrobial stewardship involves organisational and healthcare-system-wide action to preserve the future effectiveness of antimicrobial medicines.
Laboratory services contribute by providing:
- timely and reliable results;
- rapid communication of significant findings;
- organism identification;
- antimicrobial susceptibility testing;
- resistance-mechanism detection;
- cumulative antibiograms;
- selective or cascade susceptibility reporting;
- diagnostic guidance;
- support for antimicrobial review;
- surveillance data.
Host-response tests may strengthen stewardship by reducing uncertainty when bacterial infection is unlikely. However, a test only improves prescribing when it is integrated into a clearly defined clinical pathway.
Simply introducing a new biomarker does not guarantee safer antibiotic use.
The service should monitor whether testing changes:
- antibiotic initiation;
- choice of antibiotic;
- duration of therapy;
- time to appropriate treatment;
- hospital admission;
- length of stay;
- repeat testing;
- patient outcomes;
- adverse events.
The Biomedical Scientist’s role
Biomedical Scientists contribute far more than operating analysers.
Their responsibilities may include:
- assessing specimen suitability;
- performing and monitoring quality control;
- recognising analytical interference;
- validating unexpected or critical results;
- authorising results;
- communicating urgent findings;
- advising on further testing;
- maintaining equipment;
- investigating quality incidents;
- supporting clinical interpretation;
- contributing to antimicrobial stewardship;
- evaluating new diagnostic technologies.
As host-response and gene-expression testing develop, Biomedical Scientists will increasingly need to understand algorithms, software validation, data interpretation and diagnostic governance.
The scientific question is no longer limited to whether a single concentration is accurate.
Laboratories must also ask:
- Was the algorithm validated in this patient population?
- How were uncertain cases handled?
- Does the model perform consistently across sites?
- Could treatment or immunosuppression alter the response?
- What action should follow each interpretation category?
- How will software updates be controlled?
- Is the test improving patient care?
These questions are central to safe laboratory practice.
What should the general public understand?
Antibiotics treat susceptible bacterial infections. They do not treat ordinary viral infections such as most colds and uncomplicated viral respiratory illnesses.
However, symptoms alone may not reliably identify the cause. Healthcare professionals may need to assess the patient and use laboratory tests where appropriate.
A decision not to prescribe antibiotics does not mean that an illness is being ignored. It may reflect evidence that antibiotics are unlikely to help and could cause harm.
Equally, a negative rapid test does not always end the investigation. Further assessment may be necessary if symptoms are severe, persistent or worsening.
People should seek urgent medical assessment for warning signs such as:
- severe difficulty breathing;
- confusion;
- unusual drowsiness;
- blue, grey or markedly pale skin;
- a non-blanching rash;
- severe dehydration;
- persistent chest pain;
- rapidly worsening illness;
- signs of sepsis.
Frequently asked questions
Can CRP confirm a bacterial infection?
No. CRP provides evidence of inflammation but cannot independently confirm that bacteria are responsible. It must be interpreted within the clinical context.
Does a positive viral PCR mean antibiotics are never needed?
No. Viral detection does not exclude bacterial co-infection or a secondary bacterial complication.
Is procalcitonin better than CRP?
Procalcitonin may be more closely associated with systemic bacterial infection in some settings. However, neither marker is perfect, and their clinical value depends on the population and pathway in which they are used.
Can blood tests identify the exact bacterium?
Host-response blood tests cannot. Culture, PCR, antigen detection, sequencing or other microbiological methods are required to identify an organism.
Can laboratory tests prevent antimicrobial resistance?
Laboratory testing alone cannot prevent antimicrobial resistance. However, accurate and timely results help clinicians select appropriate treatment, avoid unnecessary antibiotics and review therapy earlier.
Will artificial intelligence decide whether antibiotics are prescribed?
Algorithm-based tests can support decisions by identifying patterns that are difficult to interpret manually. Responsibility for prescribing remains with qualified healthcare professionals who must consider the whole clinical picture.
Conclusion
Distinguishing bacterial from viral infection is one of the most important and difficult questions in diagnostic medicine.
Traditional methods such as culture and PCR look directly for pathogens. Biomarkers such as CRP and procalcitonin examine the inflammatory response. New multi-protein and gene-expression tests analyse broader immune patterns and may provide faster, more detailed information.
No single test gives a perfect answer in every patient.
The strongest approach combines:
- clinical assessment;
- appropriate specimen collection;
- direct pathogen testing;
- host-response biomarkers;
- antimicrobial susceptibility testing;
- professional interpretation;
- review of the patient’s progress.
For Biomedical Scientists, this field demonstrates how laboratory medicine is evolving from measuring individual biomarkers towards integrating microbiology, immunology, molecular science, bioinformatics and clinical data.
These developments may improve antimicrobial stewardship, but their value depends on proper validation, quality assurance and responsible use.
The laboratory does not simply produce results. It helps transform complex biological evidence into safer patient care.
Suggested references
- National Institute for Health and Care Excellence. Suspected acute respiratory infection in over 16s: assessment at first presentation and initial management. NICE guideline NG237. London: NICE; 2023.
- National Institute for Health and Care Excellence. Antimicrobial stewardship: systems and processes for effective antimicrobial medicine use. NICE guideline NG15. London: NICE; 2015.
- Schuetz P, Wirz Y, Sager R, et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: an individual patient data meta-analysis. Lancet Infectious Diseases. 2018;18(1):95–107.
- Huang DT, Yealy DM, Filbin MR, et al. Procalcitonin-guided use of antibiotics for lower respiratory tract infection. New England Journal of Medicine. 2018;379:236–249.
- van Houten CB, de Groot JAH, Klein A, et al. A host-protein-based assay to differentiate between bacterial and viral infections in preschool children. Lancet Infectious Diseases. 2017;17(4):431–440.
- Papan C, Argentiero A, Porwoll M, et al. A host signature based on TRAIL, IP-10 and CRP for reducing antibiotic overuse in children. Clinical Microbiology and Infection. 2022;28(5):723–730.
- United States Food and Drug Administration. MeMed BV 510(k) decision summary: K210254. Silver Spring, MD: FDA; 2021.
- United States Food and Drug Administration. TriVerity 510(k) decision summary: K241676. Silver Spring, MD: FDA; 2025.
- Liesenfeld O, Shah J, Ghosh S, et al. Clinical validation of an artificial-intelligence-based blood testing device for diagnosis and prognosis of acute infection and sepsis. Nature Medicine. 2025.
- World Health Organization. Antimicrobial resistance. Geneva: WHO.